
By Gavin Cross, LMFT
You've heard the term. Maybe someone mentioned it, maybe you came across it while looking up therapists, or maybe you've been in talk therapy for a while and your therapist suggested it. Either way, you're wondering what EMDR actually is, whether the science behind it holds up, and whether it's something that would work for you specifically.
This is a practical guide to those questions. No mysticism, no overselling. Just what EMDR is, how it works neurologically, who it's built for, and what to expect if you try it, with specific attention to why it tends to be effective for men in particular.
The EMDR Therapy page highlights logistics, scheduling, and insurance information. This post goes deeper into the clinical picture.
EMDR stands for Eye Movement Desensitization and Reprocessing. It's a structured, evidence-based psychotherapy developed by Dr. Francine Shapiro in the late 1980s, originally for PTSD. Over the past three decades it has become one of the most rigorously studied trauma treatments in clinical psychology, with an evidence base that now covers anxiety disorders, depression rooted in adverse experience, attachment wounds, grief, performance anxiety, and chronic shame.
It is endorsed by the World Health Organization, the American Psychological Association, the American Psychiatric Association, and the U.S. Department of Veterans Affairs. That breadth of institutional endorsement is notable, when these organizations don't agree on much, but they agree on the benefits of EMDR therapy.
The core mechanism is bilateral stimulation, most commonly side-to-side eye movements following a therapist's hand or a light bar that is administered in brief sets while the client holds a target memory, image, belief, or body sensation in mind. Between sets, the therapist checks in briefly. The client reports whatever arose, sometimes a shift in the intensity of the memory, sometimes an associated image, sometimes a body sensation, sometimes nothing immediately visible. The therapist uses what emerges to guide the next set.
What this does, neurologically, is activate the brain's natural information processing system in a way that allows distressing material to be metabolized rather than stored in a way that keeps producing symptoms. The analogy the research supports: EMDR therapy mimics what REM sleep does for ordinary difficult experiences by processing and integrating them, but applying that mechanism to material that is too distressing to process through normal sleep cycles.
Talk therapy works through language and narrative. You describe an experience, your therapist helps you develop insight, reframe it, or relate it to present patterns. For many presentations this is sufficient. For others, particularly for material with a significant physiological or pre-verbal component that reaches a ceiling.
The ceiling shows up in a recognizable way: you can discuss the event clearly and intellectually. You know it wasn't your fault. You understand the dynamics. You've talked about it dozens of times. And yet the emotional weight of it, the way your body responds when it's activated, the behavioral patterns it drives, none of that has shifted. You're more informed about the problem than when you started. But you're not less affected by it.
This is not a failure of insight or effort. It's what the research consistently shows: traumatic and adverse experiences are stored in the nervous system, not just in the narrative mind. They live in the body's threat-response circuitry, in muscle tension, in autonomic activation patterns, in the implicit memory system. Language accesses one system. EMDR reaches another.
For men specifically, this distinction matters in a particular way. Many men come to therapy with significant resistance to emotional disclosure, not because they're unaffected, but because the cultural conditioning around male emotional expression runs deep. Why men don't talk about depression and the emotional masking patterns that develop instead are well-documented. EMDR doesn't require verbal fluency about inner experience. It works with what the nervous system is already doing, which makes it particularly accessible for men who find conventional therapy stalls in the first ten minutes.
The conditions EMDR addresses are broader than most people realize. The evidence base includes:
PTSD and trauma. The original and strongest application. Single-incident traumas (accidents, assaults, medical emergencies) and complex trauma (prolonged adverse experience, childhood neglect, identity-based trauma) both respond to EMDR, though complex trauma typically requires more preparation and a longer treatment arc.
Anxiety disorders. Performance anxiety, social anxiety, generalized anxiety, and the high-functioning anxiety that keeps men performing on the outside while depleted internally, all of these have neurological roots that EMDR addresses directly. The National Library of Medicine's research on EMDR for anxiety supports its effectiveness across multiple anxiety presentations.
Depression rooted in adverse experience. When depression is downstream of early adverse experience, loss, or trauma rather than primarily biological, EMDR can address the root more directly than medication or talk therapy alone. This includes the forms of depression that men most commonly present with: irritability, withdrawal, anhedonia, and chronic flatness.
Avoidant attachment and relational wounds. The early experiences that create avoidant attachment, caregiver unavailability, emotional punishment, chronic dismissal are stored exactly the way trauma is stored, and EMDR addresses them the same way. This is why EMDR is often incorporated into work with avoidant attachment in men and why it accelerates progress in couples therapy when one or both partners have significant relational history driving the current dynamic.
Burnout with trauma roots. When burnout is driven by perfectionism, early conditioning around performance, or identity-based stress, EMDR reaches the underlying drivers rather than just managing the symptoms. The connection between burnout in high-achieving men and early experience is frequently underestimated, and EMDR therapy is well-positioned to address it.
Gay-affirming trauma and minority stress. For gay clients, EMDR therapy is particularly effective for identity-based trauma: the experiences of rejection, concealment, discrimination, and internalized shame that often don't have a single discrete event to point to but have accumulated over years into a significant physiological load. The LGBTQ+ affirming therapy at this practice incorporates EMDR precisely because of how well it addresses that diffuse, chronic pattern.
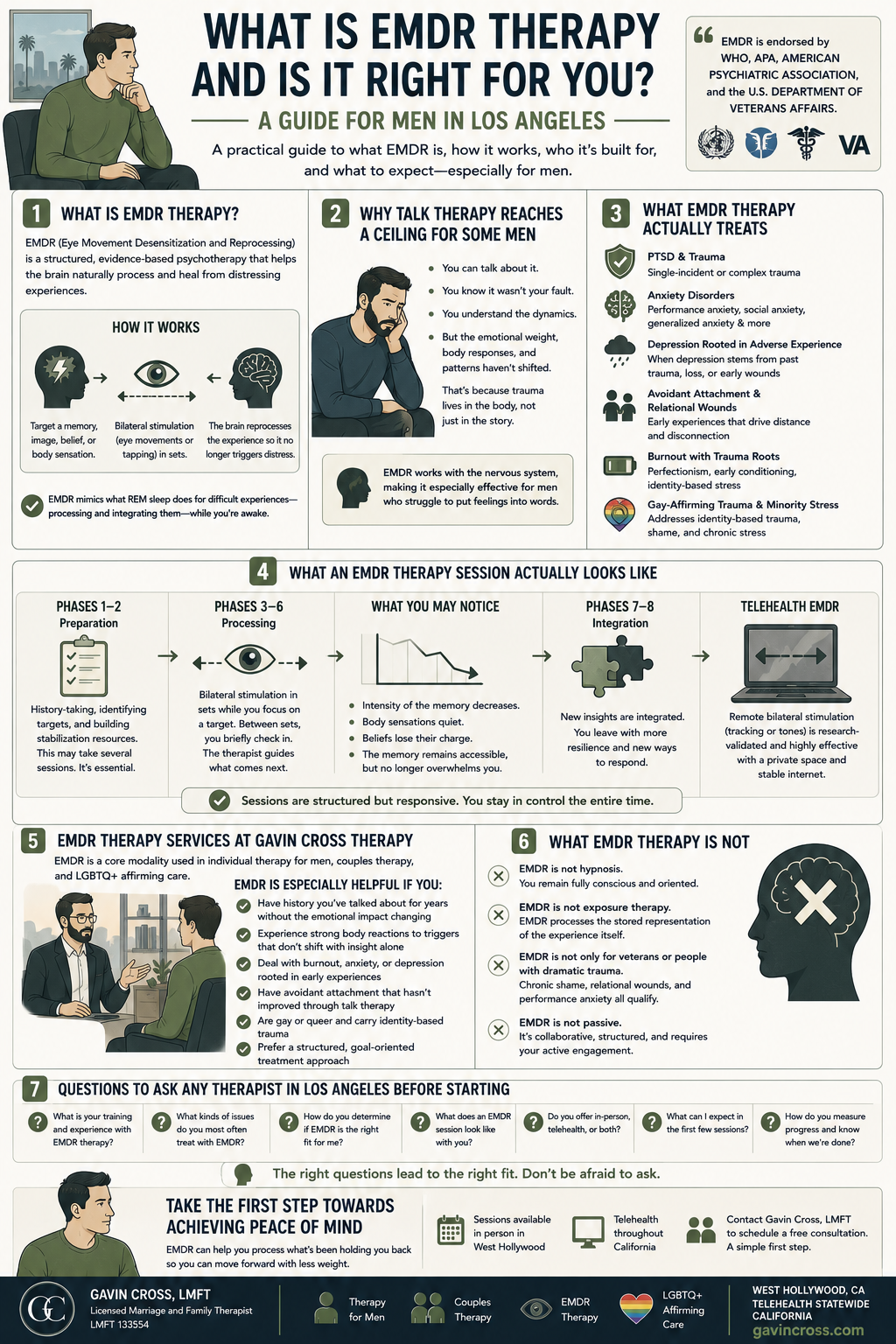
EMDR has a structured eight-phase protocol, though in practice sessions feel responsive rather than procedural. For context:
The early phases involve history-taking, identifying target memories or experiences, and establishing stabilization resources and internal anchors you can use if processing becomes dysregulating. This preparation phase is not a formality. It's clinically important, particularly for complex trauma, and it may take several sessions before bilateral processing begins.
Active processing sessions involve identifying a target, a specific memory, image, or belief, and beginning sets of bilateral stimulation while holding that target in mind. Between sets, the therapist asks a simple version of "what came up?" The client reports what arose, and the therapist uses that to guide the next set. This is not a passive process, but it doesn't require the client to narrate extensively. Much of the work happens in the sets themselves.
What clients typically notice over the course of processing: the intensity of the target memory decreases. The body sensations associated with quiet. The belief system attached to it ("I'm not safe," "I'm fundamentally flawed," "I should have handled it differently") loses its charge. The memory remains accessible. EMDR therapy does not erase memory, but it stops producing the same physiological and emotional response it did before processing.
Telehealth EMDR, which is available throughout California from this practice, uses remote bilateral stimulation tracking of a moving image on screen that has been validated in research for video-based delivery. It works. It requires a stable internet connection and a private space, but it does not require you to be in the same room as your therapist.
Telehealth EMDR, available throughout California from this practice, uses remote bilateral stimulation through a moving image on screen, validated for video-based delivery. In-person sessions use vibrating hand tappers. Telehealth sessions require a stable internet connection and a private space.
EMDR is a core modality at this practice, not an add-on. It's incorporated into individual therapy for men, couples therapy when attachment history is driving relational patterns, and LGBTQ+ affirming work where identity-based trauma is part of the picture.
The men who tend to find EMDR most useful here are men who:
A few common misconceptions worth clearing up:
EMDR is not hypnosis. You remain fully conscious and oriented throughout the session. EMDR is not exposure therapy, though it shares some overlap. Exposure therapy requires sustained contact with feared stimuli until the anxiety response habituates. EMDR processes the stored representation of the experience itself. EMDR is not only for veterans or people with dramatic trauma histories. The presenting concern doesn't need to be catastrophic to be worth addressing with EMDR including chronic shame, relational wounds, and performance anxiety all qualify.
And EMDR is not a passive experience where the therapist does something to you. It's collaborative, structured, and requires active engagement from the client, though not the kind of emotional disclosure that many men find uncomfortable in conventional therapy.
If EMDR sounds like something worth exploring, the EMDR therapy service page covers logistics, what to expect in a first session, and how to get started. The guide to finding the right therapist is a useful frame for evaluating fit more broadly before committing to a clinician.
Sessions are available in person in West Hollywood and via telehealth throughout California. Contact Gavin Cross, LMFT to schedule a free consultation. Initial consultations are a low-commitment way to ask questions and get a sense of whether the work and the therapist are the right match for where you are.
Gavin Cross is a Licensed Marriage and Family Therapist (LMFT 133554) based in West Hollywood, CA. He specializes in EMDR therapy, therapy for men, couples therapy, and LGBTQ+ affirming care, with telehealth available statewide in California.
There’s a big, beautiful world out there. You deserve to experience all it has to offer.
Let’s rediscover your strength.